There is always a lot of debate on whether to go behind or in front of the muscle with breast implants and most surgeons use both techniques. The problem with placing implants in front of the muscle is that the implant is close to the skin and rippling is quite evident. The skin can also be stretched by placing a implant that is too heavy and the implant subsequently falls down the chest leading to an orange in a sock type of appearance.
Generally a sub-glandular pre-pectoral augmentation is promoted by general practitioners and cosmetic surgeons who are not able to access the operating theatre or hospital as this type of placement can be done as rooms procedure with little sedation. A general anaesthetist is required when the implant is placed underneath the muscle as a local anaesthetic is not effective in this situation therefore Plastic Surgeons tend to use a sub-muscular placement more frequently because they have access to the hospital.
In the situation where the breast is a little droopy to start with using a sub-pectoral implant placement is not desirable as it tends to ride high and the breast falls away from the implant. Ideally implants placed in a sub-glandular position look more desirable.
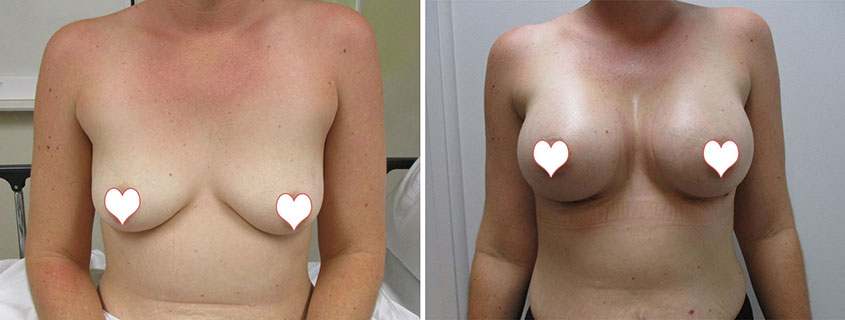
About 6 years ago I was invited to go to Rio de Janeiro with Silimed who are a large implant company to observe various surgeries that are not commonly performed here in Australia. The split muscle technique is where the pectoralis muscle is divided horizontally across the middle. For a droopy breast the top part of the implant can be placed underneath the muscle and the bottom part of the implant can be placed in front of the muscle. This means that the upper pole or top of the implant is protected by the muscle and the muscle holds the implant into position so there is less droop. When using a heavy implant the muscle stops the top of the implant falling forward off the chest wall and compresses it back against the chest. The lower half of the implant is more directly applied to the droopy breast tissue, which can expand the breast tissue and this aids as a support for the implant to help prevent the bottoming out of the implant as time goes by. This means that although it is a sub-muscular placement in the upper half there is more implant in front of the muscle than in the lower half of the breast. This would be particularly effective with a teardrop (anatomical) implant which would be used in combination with a split muscle technique to push out the lower part of the breast. This would ensure optimal results for a droopy breast without the need of a breast lift (mastopexy).
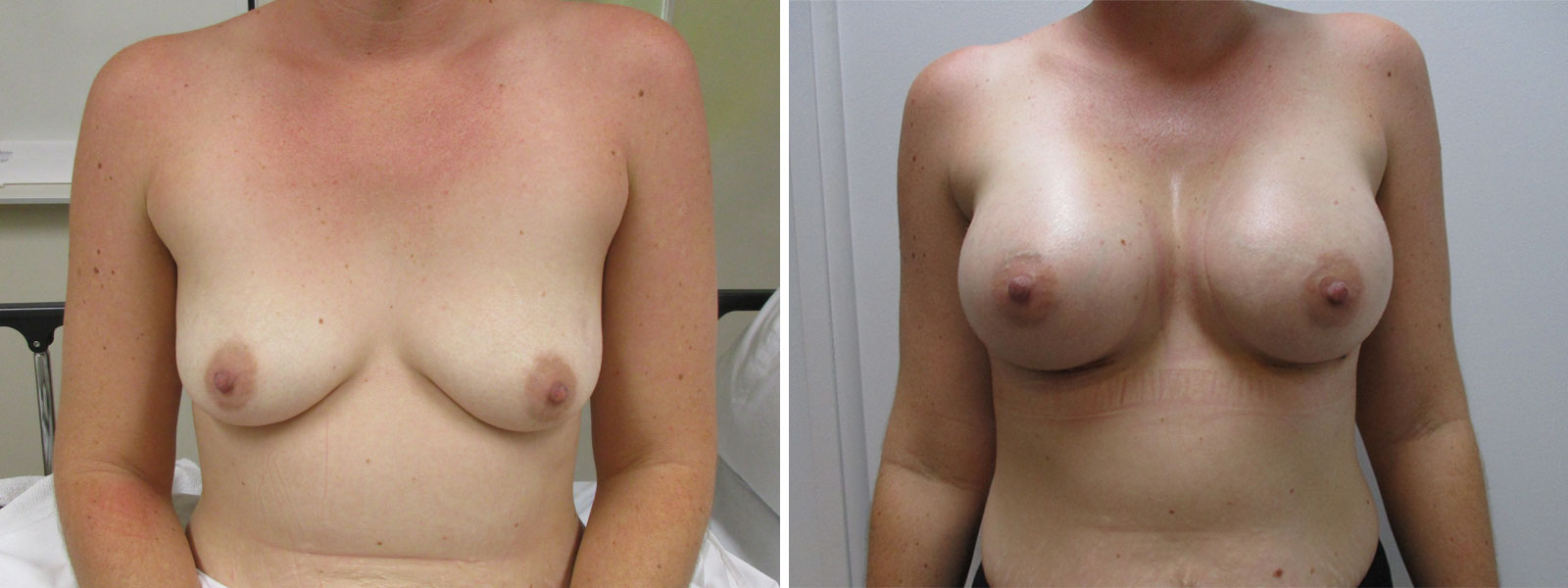
The photographs shows a patient with 475cc teardrop (anatomical) implants. I used the split muscle technique with our patient who had droopy breasts almost requiring a lift. I performed the surgery using this technique without the need of a breast lift and she is very happy with the outcome.
Further Reading Related to Breast Augmentation
- Breast Implants Perth | Breast Augmentation by Dr Guy Watts
- Breast Augmentation Implants: How To Prepare for Surgery Dr Bish Soliman
- Breast Augmentation Melbourne by Dr Carmen Munteanu
- Breast Augmentation – Breast Implants in Sydney by Dr Kernohan
- Augmentation Mammoplasty (Breast Augmentation) by Dr Jake Lim
- What is Breast Augmentation Surgery? – Anca Breahna