
So, what is the Inframammary Fold (IMF), and how does it affect breast surgery? You may or may not have heard of the inframammary fold but it plays a big part in any type of breast surgery. It is considered one of the most important aspects to the aesthetic appearance of the breast. You also may or may not be aware of the terms “upper pole” and “lower pole” which refer to the fullness of the upper or lower breast and is largely affected by the positioning of the inframammary fold. Dr Michael Miroshnik, Plastic Surgeon based in Sydney NSW took time out of his day to help us understand what these terms mean, why your surgeon should be talking about them with you at your consultation and how they affect what your final breast surgery results will be.
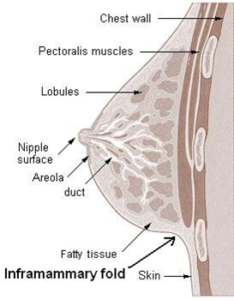
The Inframammary Fold (IMF)
Dr Miroshnik says the IMF is always on the agenda at every industry breast meeting including the Breast Masters Symposium held at the end of 2018. “The inframammary fold is always a big topic because it defines the lower pole of the breast and we all know any problems will involve the inframammary fold in one way or another, and so we as surgeons are all interested in it. Many breast procedures involve us choosing to lower the inframammary fold, and one of the main risks of this we all fear is a double bubble deformity. Simple clinical ways to define the folds would always be useful.”
Different types of inframammary folds
Dr Miroshnik says he’s identified a simple test to help figure out where a patient is with regards to their inframammary fold and how their breast surgery may need to be approached and what techniques employed to provide an ideal result. “So, when is it safe to lower the native IMF? What I’ve found is a simple straight arm test works really well. I’ve done this for thousands of patients now and it is a good way to identify the problematic folds. So, you get women to raise the arms straight upwards and then you will see four distinct groups of folds just from that simple clinical test. Type 0 is basically a non existent fold, so nature has not given this patient a fold or its very, very hard to see. We can call that la ‘blank canvas’ patient or ‘blank palette’ patient, and so it’s actually us as surgeons who are then making a decision to end the breast there and start the waist there. Obviously we can lower the fold anywhere we want in these cases, because there is no native fold”.
“Type 1 fold is where there is a fold there, but as soon as people put up their hands and their arms are raised the fold completely dissipates, you can’t see it anymore. Again that’s a very safe fold to lower because if you subject it to gravity, modern implant technology and cohesive gel will efface that fold with little else, it’s very safe.”
“Now, we get to the trickier ones, the type 2 fold. This is where a fold is moderately prominent but you don’t really know it’s a type 2 fold until the patient raises their arms. I put a number to this : ‘50% effacement’, so it’s still there, it’s gone upwards but it’s 50% less dominant, less present. You can still lower these folds but we are starting to get a bit more cautious. The surgeon may want to fat graft (to get a better result). We want to keep the lowering to a minimum – usually less than 2cm. I also strongly believe in customizing the dual plane interface to make sure that fold is completely gone and there is no muscle covering it up.”
“Then the hard ones, these are the ones you want your surgeon to detect – this is what this test is all about – the type 3 fold. It just looks like any fold, but once the patient lifts their arms up there is no change in the fold, so the fold literally raises up the same way it was before, it’s equally as distinct. They’re are the ones that may be potentially identified as problematic folds. I think, if I’m going to lower this, I can lower it, but I have to have a plan. It can be dangerous if you don’t have a plan because a double bubble deformity will happen. So what are type 3 patient options? Easy, just don’t lower it. We as surgeons need to advise the patient by explaining there are problems with lowering this fold and these are your size limits, or if we are going to lower, we have to have a plan of attack.”
Basically, a patient with smaller breasts will have less distance from the nipple to the IMF and if a surgeon does not move the IMF down when they make the incision to insert the implants, the incision and subsequent scar will end up on the actual breast when it increases in size with the implants. Lowering the IMF will allow room for the breasts to be enlarged with the implants and the scar to be hopefully tucked in to the new, concealed IMF.
Every patient is different with regards to breast size and shape, and what they want from their breast surgery. As you can see from Dr Miroshnik’s explanations of the inframammary folds, choosing a surgeon who understands the different approaches and techniques for different patients is essential to ensuring you get the best outcome. Choosing a surgeon who believes “one size fits all” will without a doubt get you into trouble. As Dr Miroshnik explains above, a certain amount of surgeon discretion and planning goes into the placement of the inframammary fold and getting it wrong can cause less than satisfactory results.
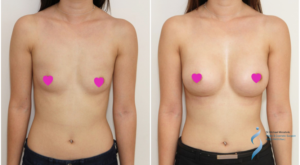
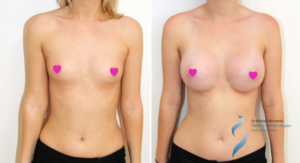
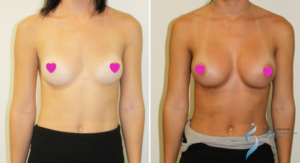
Dr Michael Miroshnik is renowned for his beautiful breast augmentations and breast surgery results, as you can see from the before and afters he shared with us. If you’d like to arrange a breast surgery consultation click here.